This will be the first in a short series of posts on my recent trip to Aotearoa. See also: Part 2: Rainbow resources from Aotearoa.
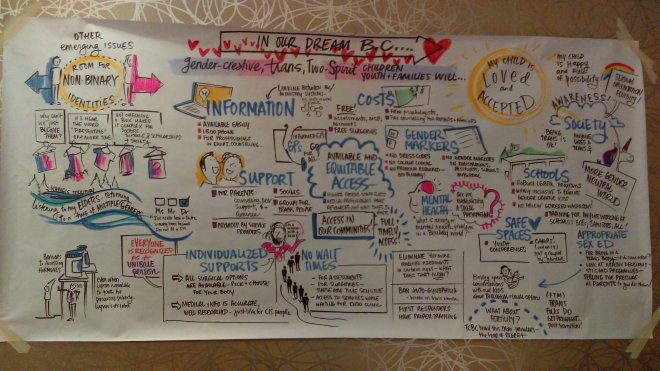
Poster in the RainbowYOUTH centre
I recently returned from a month-long journey to Aotearoa New Zealand. This trip was funded by a Rockefeller Foundation Fellowship with the School of Sociology and Social Policy at the University of Leeds.
My aim was to learn more about trans health services and community advocacy, while also sharing findings from my own research in a European context. I feel deeply privileged to have had the opportunity to meet many amazing people, who are doing a great deal of incredible work.
In this post, I share a number of resources and reflections from the trip. However, this is just the tip of the iceberg – I have no doubt that will no doubt that the experiences from the Fellowship will inform my research and thinking for many years to come.
Before I begin, I should quickly acknowledge that many readers of this blog will be unfamiliar with the word “Aotearoa”. This is a term from te reo Māori (the Māori language): it’s the current name for the islands known as “New Zealand” in English. Both are official names for the country that governs this land. For simplicity (and out of respect Māori history and culture, which long predates the arrival of Pākehā, or white European settlers) I use mostly use Aotearoa alone for the remainder of this post.
Whanganui-a-Tara / Wellington: the Gender Centre and Aunty Dana’s Op Shop
 After a brief visit to Auckland (where I recovered from the long flight) I began my trip in earnest with a visit to the capital city of Aotearoa New Zealand, on the south-west tip of the North Island. I was told that you can’t beat Wellington on a good day – certainly, the bay of Whanganui-a-Tara is one of the mostly stunningly beautiful places I’ve ever had the fortune to visit.
After a brief visit to Auckland (where I recovered from the long flight) I began my trip in earnest with a visit to the capital city of Aotearoa New Zealand, on the south-west tip of the North Island. I was told that you can’t beat Wellington on a good day – certainly, the bay of Whanganui-a-Tara is one of the mostly stunningly beautiful places I’ve ever had the fortune to visit.
My first priority was a visit to the Gender Centre. This amazing new community resource, which was founded only last year and is currently based the front room of the 128 Radical Social Centre. It is run by members of Gender Minorities Aotearoa, a group who campaign and provide information for transgender, takatāpui, and intersex people. Takatāpui is a term in te reo which “embraces all Māori with diverse gender identities and sexualities“.








Photos of 128 Radical Social Centre and the Gender Centre, taken with permission.
The Gender Centre includes a small office space, where people working for Gender Minorities Aotearoa can work on current campaigns and meet with visitors. Anyone can drop by to ask for advice or support, or pick up information. For example, the organisation has recently started running a free binder scheme. Materials on display included forms for name and gender changes, advice on accessing healthcare services, and information on the BDMRR bill.
BDMRR stands for Births, Deaths, Marriages, and Relationships Registration. Groups such as Gender Minorities Aotearoa are campaigning for non-binary recognition, and to make it possible for people to legally change the gender marker on their birth certificate without going through an expensive process involving medical oversight. Unfortunately, proposed changes have been delayed by the actions of anti-trans hate groups. UK readers will recognise the similarities with the campaign of misinformation waged against proposed changes to the Gender Recognition Act. This is not a coincidence. Anti-trans groups in Aotearoa are directly influenced by the language, aesthetics and (in some cases) the direct interventions of UK anti-trans campaigners, in what can be understood as a form of neo-colonialism.
While I was at the 128 Radical Social Centre I also visited Aunty Dana’s Op Shop. This is a second-hand clothing and accessories store run by trans and non-binary volunteers and open to people of all genders, with proceeds donated to Gender Minorities Aotearoa. It’s such a great way to raise money for campaigning, while providing an important resource and social space. It can also serve as a less scary space than the Gender Centre for people who are just coming out and looking for support. I had a great time browsing the shelves and chatting with the volunteer who was working there that afternoon.




Photos of Aunty Dana’s Op Shop. Taken with permission.
You can watch a fantastic video about the Op Shop here:
While I was in Whanganui-a-Tara I also took the opportunity to visit a trans and non-binary artists showcase at the NZ Games Festival and meet with some brilliant academics and students working on LGBTIQ research at Victoria University of Wellington. I will be sure to share their work as it is published!
Ōtautahi / Christchurch: queer art and affirmative care
I next travelled to Ōtautahi / Christchurch, taking a train down the east coast of the South Island. During this trip I began to understand the extent of the damage caused by 2010 and 2011 Canterbury earthquakes. There was evidence of huge landslides and roads were still being rebuilt. Several metres of new coastline were visible for many miles, clearly identifiable through rocks bleached white by dead organisms that once lived under the waves. The city itself is still being rebuilt. Huge building projects and areas of empty land can be found throughout the central business district, a reminder of the unforgiving power of the Earth.



Photos: day and night – urban art and public protest.
It was apparent that the people of Ōtautahi were still recovering from tragedy even before the horror of the recent neo-Nazi mosque shootings. Nevertheless, the city struck me as a great centre of culture. I am grateful to have had the opportunity to meet some amazing queer and feminist artists and heard about both radical public interventions and commissioned works. If you want to learn more about this, the websites of Jennifer Shields and Audrey Baldwin are great places to start.
During this visit, I learned about a fantastic initiative to build and publicise new public health pathways for gender-affirming care in the Canterbury region. Until recently, services such as specialist counselling, hormone therapy and surgical referrals were only available on an ad-hoc basis, and information was not easy to find. Relevant information on what services are available and how they can be accessed is now easily available, thanks to the work of the Ko Awatea gender-affirming care co-design group.
These services are still not perfect – several interventions are not publicly funded, and they still involve a certain level of medical gatekeeping. However, they represent an important step forward. Notably, I was informed that these achievements can be credited to the willingness of particularly motivated medical providers, who were prepared to put energy into working directly with trans community representatives to work for reform.
Tāmaki Makaurau / Auckland: RainbowYOUTH

The next stage in my journey was a visit Kirikiriroa / Hamilton, back on the north island. I was here for the Aotearoa New Zealand Trans Health Symposium. This will be the subject of a future blog post, so I am going to finish this piece with a look at an organisation based in Aotearoa’s largest city.
In finish my journey with a return to Tāmaki Makaurau / Auckland, meeting a number of community workers, activists and academics living and working in the city. I was especially honoured to visit the RainbowYOUTH offices and drop-in centre: a spacious explosion of colour located in an otherwise unobtrusive side street on the edge of the queer distract around K Road.
RainbowYOUTH are an organisation run by and for queer and gender diverse youth, with a remarkably long and successful history. They are currently celebrating their 30th anniversary, having been founded in 1989. The organisation’s members and executive board are all aged 27 or under. Executive advisors aged over 27 are invited to attend and speak at board meetings, but do not have voting rights. I was really impressed by this commitment to centring youth perspectives in support work and activism, something which has been missing from the UK since the dissolation of Queer Youth Network.
I was also interested in how common the language of “rainbow” community was in Aotearoa, as an addition and alternative to acronyms such as LGBTIQ. I like the way this word avoids the “alphabet soup” and potential exclusions tone of the acronym. I can also see how – like the term “gender minorities” – it can work to be inclusive both of intersex people and of takatāpui in a way that is more expansive than just attempting to rework the Western/anglophone framework of “LGBT”.















Photos of the RainbowYOUTH centre. Taken with permission.
The RainbowYOUTH centre was a wonderful building. For a long time, the organisation ran out of a very small office on Karangahape Road, but in recent years an increase in income and activity enabled a move to the new space. This features several offices, a therapy room, a large social space with a TV and gaming consoles, a library, a community wardrobe, free hygiene packs for people in difficult circumstances, and once again a whole range of resources and information. I can see how the very existence of this space is helping to create new possibilities for a generation of young people who I hope will achieve things that currently remain unthinkable.
I left Aotearoa incredibly inspired by the work and imagination of everyone I met, and am hugely grateful to everyone who helped with advice and organisation, made time to speak with me, and shared ideas and information. Ngā mihi nui!



 Wednesday 28 February
Wednesday 28 February