I’m currently helping to raise money for Isaac, a young trans man I know, and his family.* In the face of enormous NHS failings, they need your help to afford trans healthcare.
There is of course already a lot of fundraising for healthcare within trans communities. This is inherently unfair for several reasons. Firstly and most importantly, it’s wrong that people struggle to receive the care they need from state-funded providers, and pretty much all trans people across the world are discriminated against in this regard (whether or not we are talking about medical transition).
Secondly, research showsthat crowfunding tends to favour individuals with more existing social capital. People trying to raise money for their care benefit from factors such as being older, transmasculine, white, and/or well-connected on social media.
However, there are cases where we simply don’t have the infrastructure or resources in place (yet?!) to support collective fundraising. A good example of this is all minors: young trans people who are more likely to face heightened discrimination and legal barriers both to accessing care in the first place, and in attempting to circumnavigate these barriers.
I do not have the capacity to make a habit of running fundraisers. In this instance, I have known both Isaac and his family for a long time. I know that they are systemically disadvantaged due to economic factors, an inability to go public and put a face to their crowdfunder, and the intersection of transphobia, racism, and various other forms of structural oppression.
Here’s some of the blurb from the crowdfunder page about why you should support Isaac:
Isaac’s story
Isaac is a Black trans kid living in England. He is an expert baker of chocolate chip cookies, loves painting and drawing sharks, and has a budding rock collection. He’s obsessed with highland cows, and knows all the words to Hamilton.
Isaac has a very supportive family who want to help him access healthcare. However, they are in low income work, and are on universal credit.
They therefore need your help to afford care for Isaac.
NHS failings
Isaac received a diagnosis of gender dysphoria from the NHS England Gender Identity and Development Service (GIDS). However, the clinical timelines were so slow at GIDs that this diagnosis came too late for him to access any medical treatment before the clinic closed in 2024.
Like many of young people, Isaac has found the new NHS trans healthcare clinic for under-18s – the Children and Young People’s Gender Service – to be traumatic and abusive. He also has no hope of being prescribed medication there.
For more information on young trans people’s terrible experiences at NHS clinics, see Dr Cal Horton’s article, “The worst thing I ever experienced”
How much money does Isaac’s family need?
We are aiming to raise up to £8000. This is to cover the cost of the following for up to three years:
Diagnostic appointments
Subscription to a private clinic
Medication costs
Blood tests
Isaac’s family may save on some of these costs if they can find a GP who will provide shared care and blood tests. However, this is not guaranteed.
If Isaac’s treatment costs less than the money raised, any remaining donations will go towards a top surgery fund for when he is an adult.
If there is still remaining money not spent on Isaac’s healthcare, the family will donate this to fundraisers for other trans kids and/or other trans people of colour.
*Isaac, of course, is not his real name.However, the image for this campaign is a self-portrait of his future self that he drew when much younger. Isn’t it amazing?
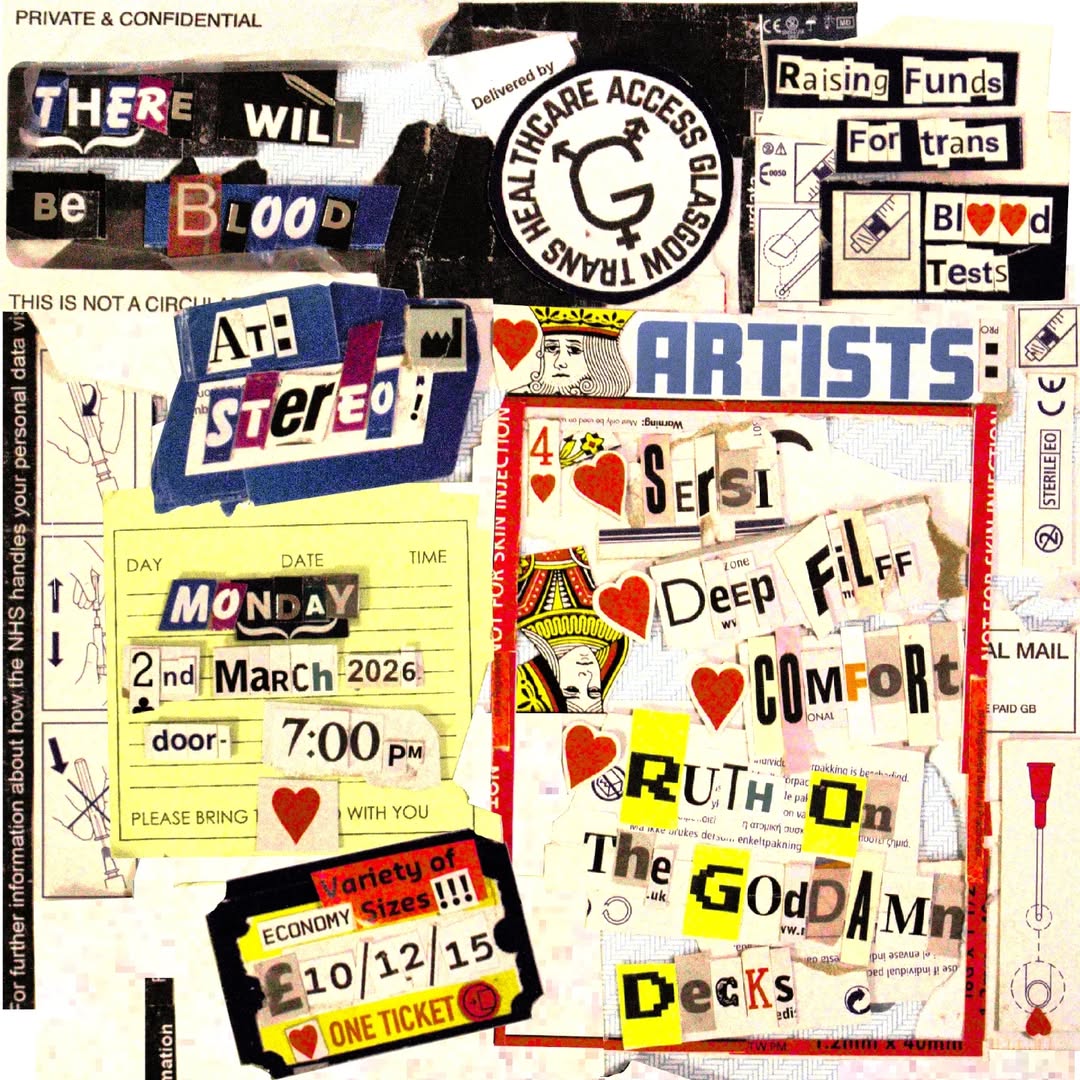
I’m super hyped to announce I will be doing a DJ set at Stereo on 2nd March 2026 – performing for the first time as ROGD.
This will be at a gig for Trans Healthcare Access Glasgow. They are raising money to provide free blood tests for trans people who have otherwise been denied healthcare by the NHS.
Much like the Glasgow Electrolysis Project (who are now running a successful clinicin the city) the very existence of Trans Healthcare Access Glasgow is both an indictment of the NHS and a credit to our community organisers. It’s depressing that the UK’s state healthcare system has so profoundly failed trans people that many GPs are now refusing to even monitor the safety and efficacy of NHS-prescribed medication. But it is also truly excellent that we are building our own new networks of medical support, which offer an alternative to the cis-led medical systems that have abused and exploited us for decades. Through the work of harm reduction groups such as Trans Healthcare Access Glasgow, we are collectively less reliant on these systems than we have ever been.
Meanwhile, I have a long history as a rock DJ but don’t get behind the decks too often these days. While I’m hoping to perform a bit more often again going forward, there’s no guarantee – so snap up those tickets while you can!
Prior to its publication, there were some concerns about the Levy Review being a sort of Cass Review for adults, leading to further massive restrictions in trans people’s access to healthcare. I witnessed active catastrophising in some quarters, with social media posts calling medication stockpiling. I don’t think this kind of rollback was ever on the cards with Levy, but I do understand why people were concerned. Trans people’s trust in the NHS and political processes is – justifiably – at rock bottom.
There were also a minority who hoped that the Levy Review might result in significant improvements to how trans people are treated by the NHS in England. I don’t think that was ever realistic either.
In reality, Levy does acknowledge some of the problems with English gender clinics, focusing especially on capacity issues, inefficiencies, and long waiting times. It offers a series of recommendations relating largely to the practical operation and delivery of gender services (the hint is in the title!) QueerAF asked me what I thought about it for their coverage of the Levy Review, and I told them this:
These measures may still result in a few improvements. NHS England hope Levy’s recommendations will contribute to “clinical effectiveness, safety, and experience”. I am not entirely convinced. But perhaps the waiting lists can be a bit shorter and fairer, especially with the opening of new clinics and introduction of a national waiting list.
Why is the Levy Review like this?
Levy did not truly seek to understand, let alone confront, the real scope of the problem in trans healthcare services, sticking instead to the very narrow scope of the brief provided by NHS England. Deeper issues he ignored include open discrimination from healthcare practitioners, as well as gatekeeping, pathologisation, and dehumanisation baked into the design of the gender clinics. These all harm patients, while also wasting clinical time and resources.
When I started my PhD on trans healthcare in 2010, such issues were not widely understood outside of certain trans community settings. That is no longer the case.
There have been multiple reviews and consultations undertaken by NHS England over the past 15 years, including in 2012, 2014-2015, and 2017-2019. There was also a review undertaken by the House of Commons Women and Equalities Committee in 2015.
Then there’s the research I undertook for that PhD, later published in my book Understanding Trans Health. Here, I argued that long waiting lists for gender clinics are not simply a result of underfunding or bureaucratic inefficiencies, but also an inevitable outcome of the gatekeeping system. By positioning trans healthcare as a specialist matter, and forcing patients to prove over and over again in psychiatric evaluations that they are “really” trans, you create unnecessary roadblocks and bottlenecks for care.
There have been a lotofotherstudies undertaken since. The most notable might be the massive, rigorous, and extremely detailed final report of the Integrating Care for Trans Adults (ICTA) project, published in 2024. This was funded by the UK government through the National Institute for Health Research, and has been roundly ignored by NHS England.
All this research and commentary highlights those same problems ignored by Levy: discrimination, gatekeeping, pathologisation, and dehumanisation.
My feeling is that neither NHS England nor Levy were interested in these issues. In fact, they are not really interested in understanding trans people at all.
It is therefore no surprise that Levy not only ignores widely-documented problems, but also repeats factually inaccurate claims, such as that the growth in patient demand for gender clinics is “not well understood”. Quite aside from what we have learned from all of the research and commentary noted above, this growth was forecast back in the 2000s by the education and advocacy organisation GIRES, in a study funded by none other than the Home Office.
The really bad stuff(and how to protect your data)
For all the limits of the Levy Review, I feel most of the recommendations are somewhat positive and may help people a bit. On balance, it’s mostly okay.
However, there are a few real points for concern.
Firstly, Levy argues that a first assessment for medical interventions should always be undertake by a psychiatrist or clinical psychologist. As all the research on trans healthcare services has shown time and time again, this is both unnecessary and unhelpful. It compounds the pathologisation of trans people, wrongly positions trans healthcare as a “specialist” matter, and creates expensive bottlenecks for treatment.
Secondly, Levy insists that gender clinic patients should be referred by GPs, and should not be able to self-refer. This is intended to help with the problem of patients ending up on a waiting list with no information for clinical staff on who they are, what they are looking for, and what their healthcare needs might be. However, the recommendation ignores the widespread issue of transphobic GPs refusing to provide referrals, as well as the fact that not everyone will have a GP (see, for example, the fact that trans people disproportionately experience homelessness, or that we are more likely to avoid healthcare providers due to justified fears of abuse). The problem Levy is trying to address could have been tackled in a more sensitive way, for example through NHS England providing a short referral form that prospective patients can fill in when seeking an appointment at a gender clinic.
Finally, there is the issue of future research. Citing Alice Sullivan’s transphobic report on sex and gender, Levy calls for more data collection on patient outcomes. Here Levy fails to acknowledge the urgent need to build trust before trans patients can be confident the NHS will not misuse our data. Moreover, as Trans Safety Networkhave noted, NHS England have committed to addressing this through expanding the role of the National Research Oversight Board for Children and Young People’s Gender Services. Trans Safety Network report that the board includes members associated with anti-trans medical groups, including the Society for Evidence-Based Medicine (SEGM), who are listed as a hate group by the Southern Poverty Law Center, and CAN-SG. It’s little surprise therefore that the National Research Oversight Board has recommended that clinicians working with young trans people attend SEGM and CAN-SG conferences, ensuring the further spread of transphobic disinformation, pseudoscience, and hate.
We also suggest you email your GIC the following to ensure your opt-out is clear and ask to have a note of this added to your care record. I do not give my permission for any aspect of my patient data to be submitted to, or collected for, the purpose of any research or non local audit without my express permission in writing being obtained in advance.
Emails should include your name, DOB and NHS Number to assist your GIC admin in finding your record. If you have been referred but not been seen by a GIC, you can still contact the GIC you were referred to.
Could it be better?
The failings of the Levy Review are not inevitable. There are numerous international models of better practice. For a strong example, see the Professional Association for Transgender Health Aotearoa’s 2025 Guidelines for Gender Affirming Care in Aotearoa New Zealand. This recommends treatment under an “informed consent” model. Here is some of their guidance on this for adult patients:
Being transgender is not a mental illness, and it does not impair capacity to consent to treatment. If a doctor or nurse practitioner has sufficient knowledge, skill and professional scope to initiate GAHT [gender-affirming hormone therapy] in an adult patient:
– There is no requirement for all people to be assessed by a mental health professional prior to starting GAHT
– For many transgender adults, GAHT can be initiated in primary care, without the involvement of secondary or tertiary care.
But we need not even look overseas for better. The Welsh Gender Service has seen a growing shift towards the provision of hormone therapy for trans people in primary care settings, supported through close collaboration with community organisations and GP practices. This has proven to provide a better experience for trans patients and has improved the efficiency of the service from an NHS perspective. The ICTAreportdescribes what this looks like in practice.
Case Study 4 in Chapter 4 reports on the establishment and initial development of regional primary care clinics, spread across Wales, which take responsibility for prescribing and monitoring HRT for trans adults following assessment at the specialist gender clinic. This is the most significant initiative we studied to address lack of integration between an assessing gender service and arrangements for prescribing and monitoring HRT. The key features are as follows. Their effectiveness and efficiency would appear to be of wider relevance to other gender services and NHS primary care commissioners.
The regional clinics were largely staffed by GPs, located within established GP practices and funded by the local NHS. They took responsibility for prescribing hormones, monitoring blood tests and titrating doses immediately following assessment, aiming to pass service users on to their usual practice after around 12 months, on the basis that their doses and prescriptions would by then be stable. This arrangement avoids the costly and damaging difficulties in communication between GICs and primary care practices over blood tests and dosage changes, experienced by many people attending other GICs. It also frees up gender specialists to devote more time to assessments, rather than review appointments for people already on hormones. Local clinicians, however, worked in an integrated way with their specialist colleagues, attending joint training on trans health care, and holding regular joint clinical consultations.
Further advantages emerging from this arrangement include the regional clinics rapidly becoming established as having GPs confident in prescribing under shared care with a GIC, whether based on a full GIC assessment or on the basis of a ‘harm reduction’ bridging prescription. These more knowledgeable GPs can then advise and educate colleagues in their own and neighbouring practices. Above all, both service users and GPs involved in these regional clinics were enthusiastic about how they brought HRT for trans people into the mainstream of primary care. Doctors in the regional clinics helped service users deal with a range of health issues, and hormone therapy came to be experienced as part of primary care, rather than something specialised, difficult, or in any way stigmatised.
The Welsh model is still far from perfect. However, it proves that there is no need for NHS England to keep asking the same tired questions and presenting the same tired answers. Yes, we deserve better than the Levy Review: but more importantly, positive change is both realistic and possible.
Last month I returned to the fabulous Red Medicine podcast to talk all things Wes Streeting. I joined the socialist writer Jonas Marvin and host Sam Kelly to discuss the UK Secretary of State for Health and Social Care’s political background, possible motivations, and current challenges.
Red Medicine always offers a great deep dive into health-related topics of the day. Streeting’s alignment with transphobic pseudoscience and conversion proponents means that obviously I had a lot to say about his impact on trans healthcare. However, our conversation was offered a great opportunity to grapple with the wider context of Streeting’s ideology and actions, discussing wider matters such as class, party politics, and trade unionism: highly relevant given current discourse around the proposed strike by resident doctors! I also talk a little about my encounters with Streeting in the 2000s, back when I was a campaigner with the National Union of Students’ LGBT and Women’s Campaigns.
You can listen to Red Medicine through all the major podcast platforms – or through the link below.
You can also hear me talking about the Cass Review on a previous episode of the podcast in June 2024.
This week I took the long train down to the south of England for my friend Robyn’s funeral. She died very suddenly three weeks ago, aged just 32.
Robyn gave so much love to the world, and was so loved in turn. Around a hundred and fifty people crammed into a small building for the service. There weren’t enough seats for everyone, so many stood at the back and sides of the room. I sat on the floor. More attended online.
We shared stories from Robyn’s life, learned from each other, cried together. Like many funerals, especially for young trans people, it was absolutely gutwrenching. It also helped move us towards closure. It was good to be in community together, to think and speak not just of Robyn’s past, but of our collective futures. Robyn lived life to the absolute maximum. Surely we could take inspiration from her example.
Robyn at Manchester Punk Festival 2024. Photo by Chris Bethell for The Guardian(!)
After the funeral, I stayed the night with queer friends in rural Surrey. We went for a curry, toasted Robyn, caught up about our lives. We talked about work and about books and about art and about holidays we wanted to take. That evening I felt tentatively more at peace with the world.
And then I looked at my phone. And I learned that another young friend, Jessica, had also just died.
***
It’s a shit time to be trans. Many people are saying this.
But then again, when has it not been a shit time?
Eight years of moral panic have taken an enormous toll. In the UK, as in many other countries, our civil rights and our access to public services, public spaces, and public life are all being rapidly rolled back. Politicians and influencers fall over themselves to promote anti-trans violence and praise one another’s incendiarytakes. We are less safe at work, at home, in hospitals, in schools, and in the streets.
Trans people often die young, including too many of my friends. Sometimes (all too often) we die by suicide, driven to despair in a world full of hate and malice. Sometimes (mercifully less often in the UK) we are murdered, usually in incredibly violent ways. Other times, it’s more complicated. I think of Denise, who died a sudden death from melanoma. I think about Elli, who died of Covid-19. And now I also think about Robyn and Jessica, who each died suddenly of apparently natural or accidental causes.
These days, the high rate of untimely trans death can feel like a consequence of the trans panic. Certainly I believe it’s making things worse. However, this phenomenon pre-dates the current political situation. Trans people disproportionately died young in the 2010s, at the time of the so-called “tipping point“. Trans people disproportionately died young before this too. Sociological theory can tell us why.
A decade or so ago, I worked for a couple of years in Warwick Medical School. I was there to teach medical students about social determinants of health. The basic concept is that our general health is affected enormously by the context in which we live. This includes factors such as the resources and services we do and do not have access to, and barriers we might face in attempting to access healthcare services or otherwise look after ourselves
So, it’s not a coincidence that – for example – life expectancies are shorter in poorer neighbourhoods, or that Black women are more likely to die in childbirth. There is nothing inevitable or biological about any of this, something intrinsically different about poor people or Black people. The issue is that entire groups of people are more likely to experience particular kinds of illness, and more likely to die of things others might survive. This is because of the social disadvantages they face, and because of the discrimination they experience at the hands of bigoted doctors and nurses.
There is a massive scientific literature on social determinants of health. I’ve contributed to it myself, co-authoring a recent study showing an association between transphobic microaggressions and poor mental health among trans people. For this reason, I know it’s no coincidence that so many of my trans friends have died untimely deaths. Trans people are more likely to have worse health because of transphobia. They are less likely to receive timely and effective treatment because of transphobia. This means when trans people are seriously ill, we are on average less likely to survive. I see this when I look at the academic literature, and I see this every day in the lives trans people I know.
I see the impact of transphobia when I look at Robyn’s life and death. Her health deteriorated significantly in her final years. She was afraid to seek help from doctors though: and for good reason, given the discrimination she and many of her friends experienced in NHS services. I wrote my entire goddamn PhD thesis on this problem.
Things were even worse for Jessica. I witnessed so many organisations and institutions in her home city of Coventry failing her time and time again. I could fill whole books with accounts of the violence done against her. She was failed by her school, her church, a political party she gave so much energy to, the council, the local hospital, the psychiatric ward, the housing association. Just last year I sat helplessly on the other end of the phone while she attempted suicide, doing the best I could in this moment to ensure that she was not alone.
The institutional failings experienced by Robyn and Jessica and so many others are the result not just of ignorance, but of actively malicious transphobia and transmisogyny. I believe these factors contributed significantly to their untimely deaths.
How can any of us expect to find hope and purpose in the face of such violence?
***
In recent months I have noticed an uptick in trans doom-posting. By this I mean trans social media posts, blog posts, and videos which dwell entirely on negative feelings and convey a sense of hopelessness.
A prominent example is Shon Faye’s recent essay, well, it’s over, which she describes as “a brief eulogy for the ‘trans rights’ movement”. Shon observes that powerful transphobic movements in the USA and UK are succeeding in many of their aims. They have spread fear and disinformation far and wide, made allies of mainstream politicians and media platforms, and enacted bans on trans healthcare. Now they are attempting to criminaliseour very existence, as part of a campaign to eliminate us altogether.
Shon’s conclusion appears to be: well, that’s it. We’re all fucked.
“Today I doubt I will see another progressive measure (either in legislation or healthcare policy) put in place for trans people in my lifetime. Who knows what may yet be taken away.”
I very much empathise with her account of trying to talk about this in any way with cis friends and family:
“their instinct is to try and generate hope or minimise despair [which] typically minimises the gravity of the situation and the depth of my grief and exhaustion and fear – increasing my resentment.”
Shon concludes that she doesn’t want to hear “fucking platitudes” – “there’s time for hope later”. For now, she wants time to grieve. I’ve seen similar sentiments shared by other authors on various social media platforms, including posts from extremely popular trans meme accounts.
I understand intimately where all of this is coming from. Just look at everything I said earlier about social determinants of health. I recognise the violence we are subject to, and its costs. This post too is written from a place of deep grief.
But there is also the question of where and how we grieve. We do need space to vent and to despair. But we also need space to process, and figure out what happens next. Ideally, we need places and times we can do this collectively, rather than just being isolated as individuals. Robyn’s funeral offered this.
I’m not saying we shouldn’t talk about what is happening to us. What I am concerned about is the individualising effect of public platforms, and the parasocial relations we hold with high-profile accounts. We tend to consume doom-posting on our own, on a phone. We often have no-one to process it with, and little context beyond the content in front of us. In this way, doom-posting offers only a partial account of reality, and no way out from despair.
And there is a way out. We find it in community.
***
Look, I have a great deal of respect for Shon Faye. I have a hard enough time navigating the consequences of my own very minor microcelebrity. Shon has to tackle a great deal more attention: from trans people looking for someone to idolise and/or tear down, from cis readers who project heroic expectations onto her, and from haters who see her as the antichrist or something. She’s great on camera, and a brilliant writer. I would recommend her book The Transgender Issue to literally any cis reader. I also recognise that her blog post comes from a place of incredible pain.
At the same time, I am concerned that many trans people and allies are putting way too much energy into engaging mainstream institutions and liberal systems on their own, individualistic terms, rather than looking to the alternative power and support we can build in our communities. Notably, a lot of Shon’s post talks about civil society, legislation, lobbying, and the role of organisations such as Stonewall. This is definitely a realm in which “trans rights” face a seemingly terminal decline. But it is also not the first place I would look for real, grounded hope.
You can find a similar energy in Jules Gill-Peterson’s dire essay Reject Trans Liberalism, which is referenced by Shon. Jules’ piece simultaneously criticises the trans liberation movement for being about more than transition, while also insisting that preparing ideologically sound documents for the US supreme court is a radical act. It posits a false and ahistorical dichotomy between transsexuals (good, pure, radical) and transgenders (bad, elitist, liberal). The essay does not consider how gender diverse people might work together or support one another across our differences. This contrasts with existing critiques of trans liberalism already advanced by activist-scholars such as Nat Rahaand Mijke van der Drift. Again, don’t get me wrong, I’m a huge fan of Jules’ previous work. But as trans people, and especially as trans women, we owe each other so much more than this.
Now, I’m hardly without fault. This very blog is replete with examples of myself and others putting untold hours into lobbying politicians, participating in public consultations, advising the National Health Service and so on and so forth. In her post Stepping Over The Line, Josie Giles, who once again I admire greatly (look, I just fucking love trans women) argues that:
“Theoretically, an army of well-resourced energetic activists could simultaneously engage in state-centred advocacy and also do grassroots politics. In practice, it doesn’t happen. In practice, state-centred pseudo-organising dominates the social media feeds and the limited energy reserves of an already depleted community, and absorbs what little money is available to pay for the salaried self-licking ice-cream cone of the lobbying profession.”
Sick burn!
Meme acquired via one of them social media platforms we’ve all heard so much about.
I do disagree with Josie a little. Unlike Shon and Jules and also Josie, I transitioned in the early 2000s. This was well before the tipping point, and before most trans civil rights even existed in law. I remember how we fought successfully for changes that genuinely improved many people’s lives. I feel it will always be worthwhile to use what levers we can to minimise the harm caused by those who have power over us. Lobbying is the most accessible form of activism for some people. I still have an auto-reply on which encourages every damn cis person who emails me at work to contact their MP.
But Josie is completely right that many if not most trans people can and should be putting a lot more of our energy into grassroots politics. This must necessarily involve re-imagining what our worlds could look like, using what we already have as a basis from which to build. I know from lived experience that we can not only survive in the absence of certain civil rights and recognition, but also see material improvements in our lives when we come together. I met Jessica because we built trans-led community services in Coventry from the ground up.
Similar points are made by Roz Kaveney, who first came out over 50 years ago. In her criminally underrated 2022 poetry collection, The Great Good Time, Roz does reflect on the violence faced by young trans women in her youth. However, she also details the vibrant lives they lived together, the joys they experienced, how they shared housing and clothes and had each others’ backs. In a short forward to the book, she notes:
“I observed a lot of bleakness creeping into trans social media and thought it my job as a community elder to remind young people that things have been, if not worse, then at least as bad in different ways”.
As Josie states in Stepping Over The Line, white, middle-class trans people in particular need to understand in this current moment that we are as disposable to the ruling classes as any other minoritised individual. Our strength lies in practical solidarity with others subject to the violence of corporations, fascist movements, and the state. To once again reiterate the point, we need to be in community with one another.
Both Robyn and Jessica’s lives offered perfect models for this.
***
Every single speaker at Robyn’s funeral talked about how much time and energy she put into punk and folk music, building and fixing things, and caring for others. She was a loud, proud butch who was incredibly committed to sustaining community wherever she went. When she saw a need, she sought to meet it. Many of us only wished that she was better at asking for or accepting help herself.
If a trans person needed somewhere to stay, Robyn would put them up. If a trans person needed to move house, or was being evicted or was fleeing a violent relationship, Robyn would turn up with a van. If a trans person was having trouble at work, Robyn would show up online or in person with sensible advice. This attitude inspired Robyn to volunteer with groups such as Reading Red Kitchen, a grassroots project which provides a social foodbank and free community meals for asylum seekers experiencing food poverty. For Robyn, radical politics could never simply be about slogans and demonstrations: it was about cooking, connecting with others, and washing the dishes.
None of this is to say that Robyn was never found at a protest: quite the opposite. When I lived in the south we co-founded Trans Liberation Surrey, a collective which worked to oppose transphobia in a county hardly known for its activist movements. My most treasured memory of Robyn is from this time, when we attended a small anti-fascist demonstration in Wokingham. A coalition of neo-nazis, anti-vaxxers, and climate conspiracists descended on the town to protest a drag queen storytime event for young children. Robyn and I joined other locals outside the library to wave rainbow flags and play upbeat music, enabling families to attend the event without disruption.
Trans Liberation Surrey, at Surrey Pride 2021.
Jessica was also extremely motivated to help others, in spite of her own difficult circumstances. Like Robyn, she was a committed trade unionist. For many years she was also involved in a small political party, before eventually being ejected for challenging the leadership. Her motivation for this was a genuine belief in the possibility of positive political change, and in the potential for people to come together and make that change happen. Later in life she would rediscover her Christian faith as alternative vehicle for community action.
After hearing of Jessica’s death, our mutual friend Charlotte reached out, and we asked one another how we knew her. It turned out Charlotte had also been a member of that political party, and reconnected with Jessica several years later as they both sought new ways to make a difference in the world. In turn, I explained how Jessica and I met while lived in Coventry, and was myself involved in organising trans community social events, meals, and punk nights. Charlotte and I also both knew Robyn. “Christ Ruth,” said Charlotte, “trans lives are so entangled and we often don’t even realise”.
So it is. Right now, Jessica’s Facebook wall is replete with people thanking her for being there as a friend, for providing them with advice, for helping them come out.
In a hostile world, we are everything to one another. In the face of the most horrific hate, our love is so powerful. Such love survives death.
Selfie taken by Jessica.
***
This is where I find hope. At protests and demonstrations, sure, but more importantly in the contexts where we give each other’s lives meaning.
I find hope in community meals, mutual aid, queer bars and queer bookshops and queer gigs. I find hope in small parties, in big Pride events, in quiet meetings at work, in food pantries. I find hope in housing projects and healthcare projects, and in the Glasgow Electrolysis Project, which has created actual jobs for trans women and a vital new service for hundreds of us across the city. We know we are failed constantly by mainstream institutions: rather than seek incremental change, is it not time to re-imagine the clinic, re-think the workplace? Our problems will not be solved by refusing to engage with existing services, nor by creating trans charities that replicate existing hierarchies. We need to find ways to build something new entirely.
I find hope in the fact there are more of us out than ever, more connected than ever. These collective endeavors are all so much more important than anything I personally might write, any research I might do, and certainly any “progressive” policy I might influence.
Doom-posting and finger-pointing cannot deliver any of these things. We need to take the time to connect with one another, especially outside the internet. Yes we need to grieve, but we need so much more than this. We need to actively look after one another, and provide space for rest and recuperation. We need to have each others’ backs. We need to connect across difference, and not (re)create hierarchies of oppression or need.
These are no fucking platitudes. This is my life. This is the lifeblood of our shared communities. This is how we create better social determinants for our goddamn health.
On 8 February 2021, Brighton and Sussex University Hospitals NHS Trust published a series of groundbreaking resources on perinatal care for trans people, written by their Gender Inclusion Midwife team. As of March 2025, the Trust no longer exists, the midwives in question work elsewhere, and the resources page was sadly taken down – a sadly all-too common experience with NHS guidance for working with marginalised peoples.
Given the importance of these materials, for which I was part of a large team of expert reviewers, I am reproducing them on my website today for Trans Day of Visibility 2025, alongside some related resources.
I hope these will be of interest and use to anyone interested in improving perinatal care for trans people, including midwives, nurses, doctors, policymakers, commissioners, advocacy groups, and of course also families and prospective parents.
Professional guidance and protocolsby the Gender Inclusion Midwives
It’s been a long four years since the Gender Inclusion Midwives resources were published. Here, therefore, are a few additional materials that may be of help to people working in this area.
National Maternity Survey data on trans birth parents Since 2021 the Care Quality Commission has collected data on gender modality as part of its annual National Maternity Survey. The most recent findings indicate a significant rise in the number of men and non-binary people giving birth since 2021, with 1.58% of 2024 respondents indicating a gender that differs from the sex they were assigned at birth. This shows that hundreds of trans people are giving birth in England every year. See: Open data > 2024 Maternity survey National tables > page g9.
Improving Trans and Non-Binary Experiences of Maternity Services (ITEMS) 2022 report published by the LGBT Foundation, looking at the findings of an English study on the experiences of 121 trans people who conceived and gave birth. It found that many trans birth parents do not feel safe sharing their identity in perinatal services, with a large proportion not feeling comfortable to access any support at all from an NHS or private midwife.
Trans Pregnancy Project website I reviewed the Gender Inclusion Midwives resources as part of my work on the Trans Pregnancy Project, which was an international study of trans people’s experiences of pregnancy and childbirth. This year we launched a new website. This includes links to all our peer-reviewed publications, on topics including conception, pregnancy loss, midwifery, gender and embodiment, domestic violence, racialisation, and media representation.
Caring for Everyone: Effective and Inclusive Communication in Perinatal Care One of the key recommendations of the Gender Inclusion Midwives’ guidance on Gender Inclusive Language in Perinatal Service is the adoption of “additive” language. This approach acknowledges male and non-binary birth parents alongside mothers, rather than simply replacing woman-centred language with a gender-neutral approach. This 2025 academic article by Matthew Cull, Jules Holroyd, and Fiona Woollard provides advice on a “pluralist” approach to language, which builds upon the additive model by offering a more contextual approach. It includes clear examples of what best practice can look like.
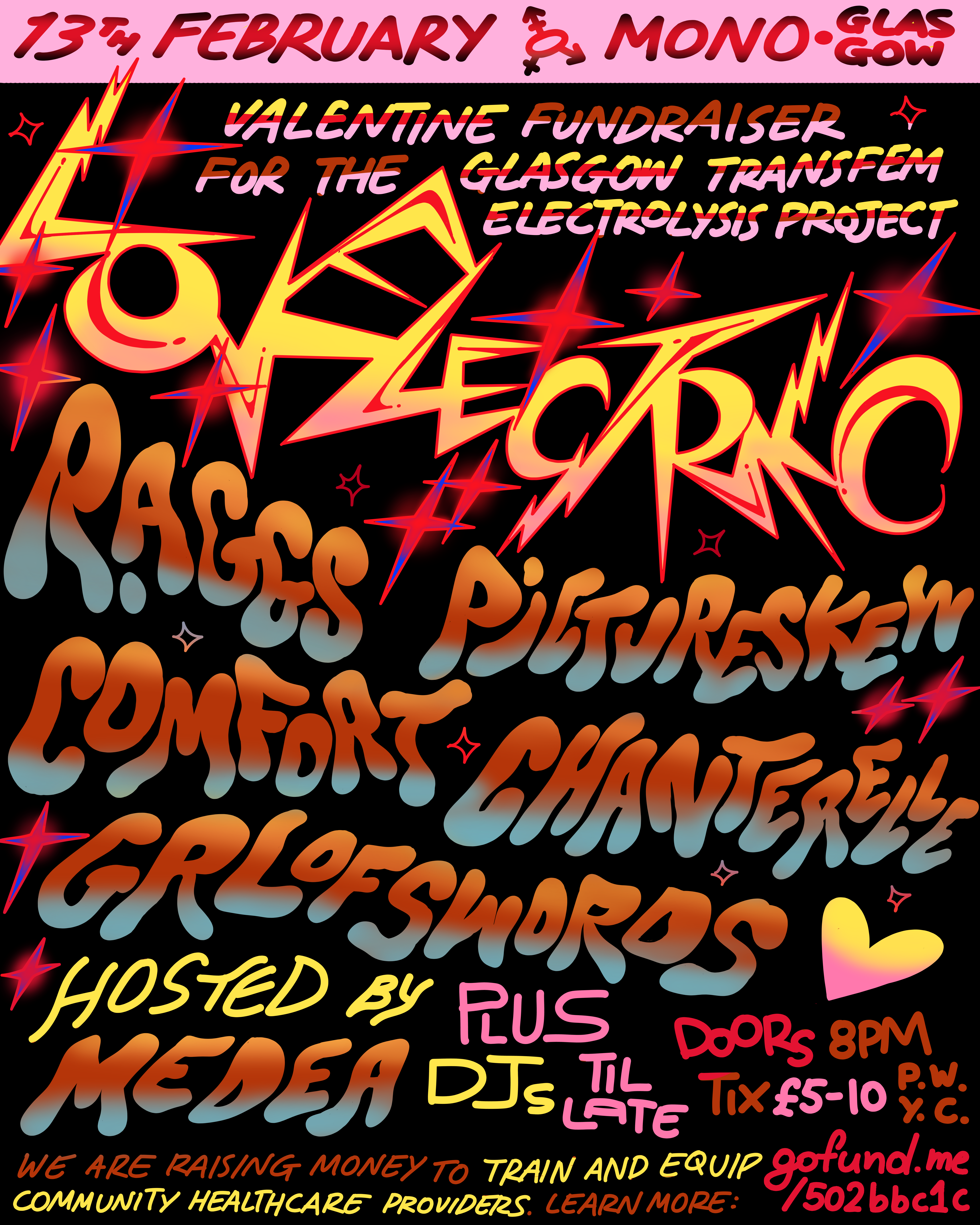
Last year I joined the Glasgow Transfem Electrolysis Project, a super cool initiative which is raising money to train and equip two community members as electrolysists. Building on the example of Electrolysis by Siobhan, who opened her service off the back of a similar project in Manchester, the project’s aim is to ensure affordable and safe hair removal for trans women and non-binary people.
In an era of continued NHS failings and civil rights rollbacks, it’s important to be reminded of the power that lies in coming together as a community and working towards a common goal in our collective interest. Hateful policymakers and journalists can never take that away from us.
You can donate to the fundraiser here. We are also running LOVE ELECTRIC, a gig at Mono in Glasgow on Thursday 13th February, with pop, folk, punk, and drag artists. If you’re local, please come by to learn more about the project, and see some incredible live performers! I’m really excited for what’s going to be an amazing night.
In early September I recieved an email from the Department for Health and Social Care, inviting me to participate in a closed consultation on the Labour government’s proposed extension of the Tory ban on puberty blockers. The deadline was 1st October 2024.
September was already extremely busy. I started the month at the International Trans Studies Conferencein Chicago, and ended it at the WPATH Symposium in Lisbon. In the meantime I was faced with various writing deadlines, administrative tasks, and the start of a new teaching semester. The small number of other academic experts and voluntary organisations who were also invited to respond no doubt faced very similar challenges with the short notice and unforgiving deadline.
Nevertheless, I scrambled to respond. Like Cal Horton, I regard government consultations on trans healthcare to be inherently abusive at this stage; as I wrote to the Nuffield Council on Bioethics in 2018, “we respond not with hope or optimism, but in fear. This is the power you wield over us”. Given the turgid vibes found in recent political discourse, I also held little hope of a long-term ban being prevented. However, it seemed worth using what little prestige I have as an academic to at least try to encourage the government to listen to actual evidence.
Trans Writes are now reporting that an extension of the ban until 2027 is on the cards for Britain, following a unanimous vote on the same by the Northern Ireland Assembly. With this in mind, I am now publicly sharing the evidence I provided in the closed consultation, plus slides from an oral presentation to the Commission on Human Medicines, who advised the Government.
I don’t think for a moment that sharing these materials will change anything in the short term. However, I feel it is important to put them in the public realm now for the sake of transparency.
Going forward, I hope the work that many of us have done in building and sharing an ethical base for the ethical provision of trans healthcare will make a difference. In the meantime, there is an important lesson here about relying on existing, unequal systems of power and control. As Nat Raha and Mijke van der Drift argue in their new book Trans Femme Futures, making demands of institutions leaves the power in their hands. It is more important than ever for trans people to build power and knowledge within our own communities, in collaboration with others.
We have survived worse in the past by sharing information, ideas, and life-changing medication between us, and we will do so again.
The book is currently on offer from the publisher, SUNY Press. If you order by 6th December you can buy the book for 50% off with the code HOLIDAY24. That means the paperback edition will come to $22.47 for those in the USA, or £24.12 with postage for buyers in the UK.
I should clarify also that, as usual with academic books, I won’t personally be seeing a penny from its sale. So if you’d like to read this publication, please do get it at a bargain price if you can!
I’m really grateful especially to Noah Adams for leading on the process of both our 2017 article and new book chapter. I first met Noah, along with Jaimie and Asa , at the 2016 WPATH Symposium in Amsterdam, which saw the presentation of numerous extremely unethical studies on trans and intersex people. I learned a great deal very fast at that symposium, and through the subsequent writing process with Amrita, Danielle, and Kai.
Most importantly, I learned that it is possible to change research and practice for the better through interventions that centre community perspectives, mutual learning, and our collective responsibilities to one another. This is an important thing to bear in mind in our current age of disinformation and the abuse of scientific discourse: while abusive practices have a long history in trans medicine and medical research, another world is possible.
This morning I logged into instagram and watched, transfixed in amazement and worry, as a young person scaled the walls of the Department for Education.
The aspiring spiderman is part of the activist group Trans Kids Deserve Better. At the time of writing they are staging a multi-day protest at the Department for Education building in London, for the right to a safe and inclusive education.
Watching the video, I fear for Squirrel, the anonymous activist who is genuinely risking their life to stop government employees from taking the group’s banner. It’s very apparent that Squirrel is a skilled climber who knows what they are doing – equally, one wrong move could result in a deadly drop to the concrete pavement. This is not safe.
But of course, the entire reason this protest is happening is because young trans people are not safe.
Trans Kids Deserve Better launched their campaign for youth autonomy, safety, respect, and inclusion in July, from a dramatically high ledge of an NHS England building. In an interviewwith Jess O’Thompson for Trans Writes, the emergency doctor and children’s TV presenter Dr Ronx Ikharia argued that “our young people deserve better than suffering, and shouldn’t be scaling walls”. But they added that for this to happen, trans kids must be “believed, supported, affirmed, and loved”.
And this is the crux of the issue. Under the Conservative and Labour governments, we have seen a policy environment in which teachers, doctors, therapists and parents are actively discouraged or prevented from believing, supporting, affirming, or loving young trans people. Instead, families face prison sentencesfor supporting young people’s continued access to medication, NHS England is expanding the provision of state-funded conversion clinics, and a growing number of schools are refusing to allow even the discussion of trans experiences.
Trans kids are not safe because they have been entirely failed by the adult world. They have been failed by politicians, failed by civil servants, failed by the NHS, failed by the voluntary sector, failed by researchers, and in many cases also failed by their doctors, teachers, and parents or carers. This is why the activists from Trans Kids Deserve Better are literally scaling walls in their fight for an actual future.
Looking at the challenges facing young trans people, it can be easy to lose hope. But the actions of Trans Kids Deserve Better show that there is a better way. Doomerism helps nobody. The successes of successive liberation struggles have come about because people have continually dared to believe that a better world is possible, and fight for it. The young people currently sat outside the Department of Education are not bemoaning what they have lost: they are insistently demanding change.
Image from Trans Kids Deserve Better
What can we do? In their conversation with O’Thompson, activists from Trans Kids Deserve Better explained that while trans adults often want to “protect” trans youth, they would rather we “amplify” them: “we don’t need sympathy, we need support”. This is a call to action, with a focus on solidarity, rather than trying to speak for young people or bemoan their situation.
Many adult trans people and allies have complained about the lack of mainstream media coverage for the actions of Trans Kids Deserve Better. But we should not simply wait for the papers or news programmes to start caring. It’s up to us to talk about what’s happening. Today’s queer and trans communities only exist at scale because we made our own media, told our own stories, and forced the mainstream to catch up.
So I encourage everyone who reads this to share the story of what is happening. Share it on social media, share it with friends and family, share it in conversations at work and in bars and in cafes and in parks and at gigs and festivals. A few days ago I was at a pub in Bath, fresh from Pride, still holding a placard that read “Ban Wes Streeting” (copied shamelessly from someone else in Glasgow a couple of weeks prior). Someone asked what Wes Streeting had done, so I told her. She was appalled, but grateful to have learned what is happening, and better informed to act. Information spreads when we spread information.
If you, like me, would rather not see young people risking life and limb by climbing public buildings, it is time to fight with them, not “for” them. Together we can build a safer world.